
Source of discussion: BJS Jan 2015
Combined vascular resection and reconstruction during hepatobiliary and pancreatic cancer surgery.

Combined vascular resection and reconstruction during hepatobiliary and pancreatic cancer surgery.
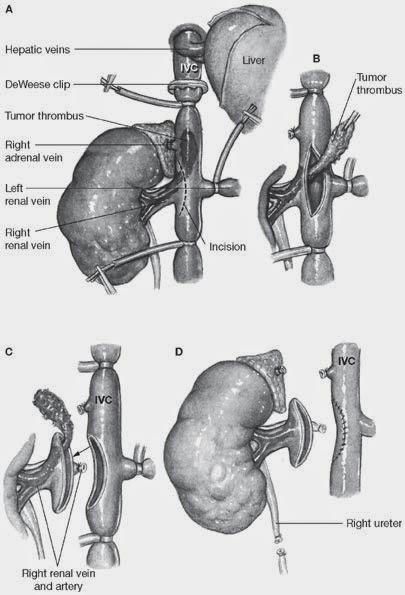
In old days, once a cancer has invaded the IVC/portal vein, it is palliative treatment only -mortality rate of resection was 6% and 5yr survival was 27% (1999). However, recent reports from major vascular centres (Leads, Paris) has shown much better outcome, with mortality rate of 11-14% and survival rate of 40% in 5yrs following IVC resection. Technical point: IVC can be ligated unless there is not enough collateral developed in before, or there is haemodynamic instability. Portal vein resection as part of pancreatectomy is now widely regarded as a safe and feasible procedure with acceptable morbidity and mortality rates. Combined portal vein resection with pancreatectomy should be considered where there is a suspicion of invasion of the portal vein to achieve clear resection margins on the basis of preoperative imaging rather than making the decision purely on operative findings. Unlike the situation with hepatic resections, combined arterial resections involving the coeliac axis, at least in the context of distal pancreatectomy, have been reported without a marked increase in surgical mortality. A variety of substitutes for venous reconstruction have been reported. Jugular, external iliac vein, great saphenous vein, left renal and umbilical veins, as well as synthetic grafts have all been used for portal vein reconstruction.here are few diagrams of the technique:



