Source: EJVES Mar2015

Finite Element Analysis in Asymptomatic, Symptomatic, and Ruptured Abdominal Aortic Aneurysms: In Search of New Rupture Risk Predictors
This is another interesting addition to the family of predictions for ruptured aneurysm. The strength of it is mainly in its derivation from real life cases and physiologic parameters, ending up in certain immediate outcome (symptomatic, symptomatic, or rupture). And yes, we are more well equipped with info if we have the FEA available with the CTA simultaneously. The problems remains in two things: the lack of adoption of such analysis by surgeons and radiologists (this is the approach of mechanical engineers anyway); and the funding (this article has one declared conflict of interest: one author is the owner/developer of the software he is claiming to work better for us) … yet again, there is no question that the future will ONLY be in such level of analysis, not in the simplified outdated one from the 1990s!!! The new generation has moved to iPhones, Maya software, adobe, smart watches, and smart cars … the technology has doubles 16 (that’s SIXTEEN) times since 1990 (as per Moore law) … so new ideas are now VERY much welcomed!!
here are few interesting findings from the paper: (images are copyrighted to EJVES exclusively).
1- note how PWRRI is significantly different in 1st vs 3rd group, even after allowing for such large CI. The PWS is also different and less widely distributed; but only for 1st vs 3rd group.

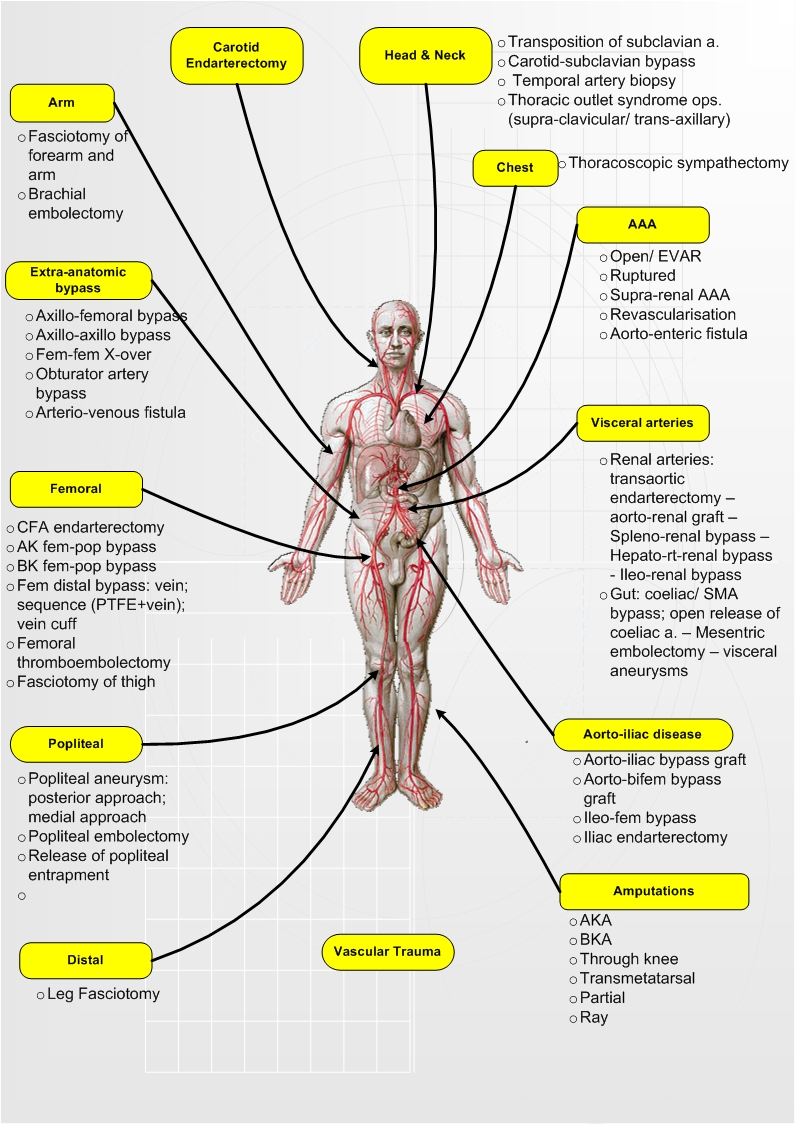
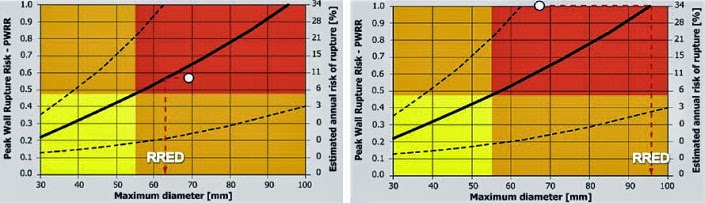
2- Note how in a case of 5.5cm, the PWS can range from 0.1 to 1.0, giving a risk of rupture from minimum to imminent! That’s dangerous indeed!! WHICH PATIENT OF OURS will rupture while we are preparing him/her to undergo a procedure! See my post on estimated risk of rupture, where more specific biomechanical factors (that are calculable by simple mathematics) gives more info on the risk of rupture compared to simple diameter measurements.