
ref:
Intra-operative Cone Beam Computed Tomography can Help Avoid Reinterventions and Reduce CT Follow up after Infrarenal EVAR
ref: EJVES Apr 2015
Fifty-one patients (44 men) were enrolled in a prospective trial. Patients underwent completion angiography and CBCT during infrarenal EVAR.
Twelve endoleaks were detected on completion digital subtraction angiography (CA). CBCT detected 4/5 type 1 endoleaks, but only one type 2 endoleak. CTA identified eight type 2 endoleaks and one residual type I endoleak. Two cases of stent compression were seen on CA. CBCT revealed five stent compressions and one kink, which resulted in four intra-operative adjunctive manoeuvres. CTA identified all cases of kinks or compressions that were left untreated. Two of them were corrected later. No additional kinks/compressions were found on CTA. Groin closure consisted of 78 fascia sutures, nine cut downs, and 11 percutaneous sutures. Seven femoral artery pseudoaneurysms (<1 cm) were detected on CTA, but no intervention was needed.
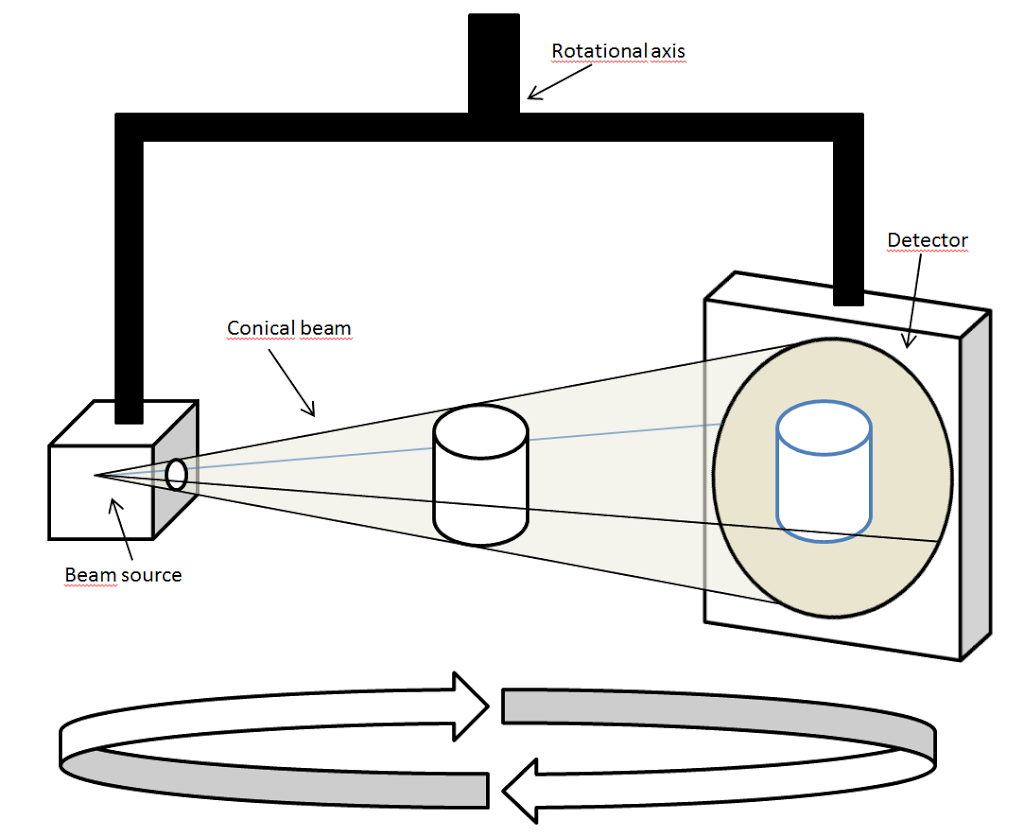
In 1996, three Italian people invented the Cone Beam CT, which went into the US market in 2001. It has become the ‘norm’ in most dental practices, as a simple means of reconstructing the X-Ray easily into 3D.
For Interventional Radiology, the patient is positioned offset to the table so that the region of interest is centered in the field of view for the cone beam. A single 200 degree rotation over the region of interest acquires a volumetric data set. The scanning software collects the data and reconstructs it, producing what is termed a digital volume composed of three-dimensionalvoxels of anatomical data that can then be manipulated and visualized with specialized software