ref: EJVES Nov 2015
Reports are emerging on using modern ‘wearable’ technologies in monitoring outcome for cluadicants. The number of patients is still low, but the idea and the statistical design and analysis are the interesting part.
In this French study, seventeen PAD patients performed two series of evaluations (T1 and T2) within a 1 month period. Each series included: a 1 hour stroll in the community with the calculation of the walking impairment questionnaire (WIQ) scores, the measurement of maximal walking distance on a treadmill (MWD on treadmill) and a 1 hour stroll in the community with GPS. Test-retest reliability of MWD on treadmill, WIQ, and GPS parameters were assessed with intraclass coefficient of correlation (ICC).
ICCs are almost perfect between T1 and T2 for greatest distance (ICC = 0.911), average speed (ICC = 0.905), and MWD on treadmill (ICC = 0.992), and substantial for the average WIQ (ICC = 0.794). Correlation of average stop durations was considered substantial (ICC = 0.691).
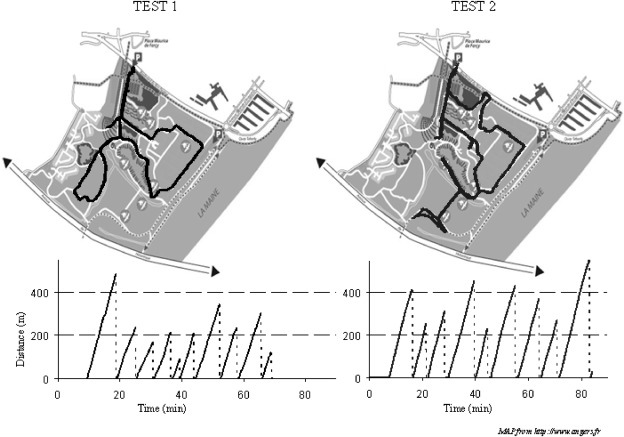
This figure provides an example of the recordings observed during the two strolls (Test 1 and Test 2) in the same patient. The figure is a copyrighted material and is not reusable. It has been used here for the sole purpose of education.