ref:
Angulation of the C-Arm During Complex Endovascular Aortic Procedures Increases Radiation Exposure to the Head
EJVES Apr 2015
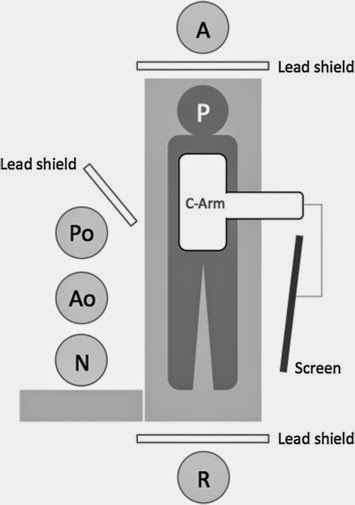
- Head dose was significantly higher in the PO compared with the AO (median 54 μSv [range 24–130 μSv] vs. 15 μSv [range 7–43 μSv], respectively; p = .022),
- as was over-lead body dose (median 80 μSv [range 37–163 μSv] vs. 32 μSv [range 6–48 μSv], respectively; p = .003).
- Corresponding under-lead doses were similar between operators (median 4 μSv [range 1–17 μSv] vs. 1 μSv [range 1–3 μSv], respectively;p = .222).
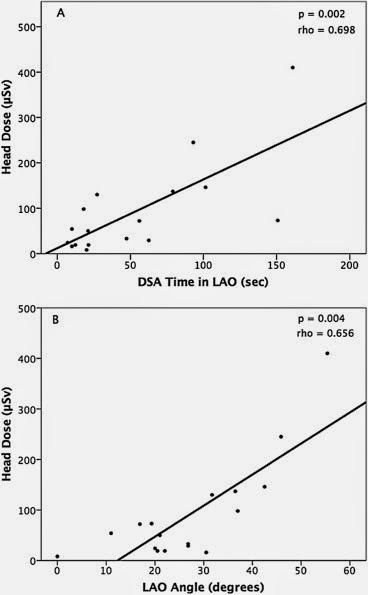
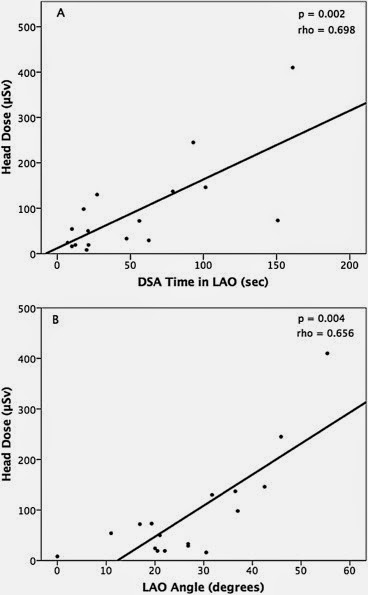
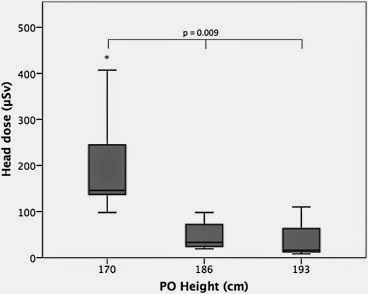
- Primary operator height, DSA acquisition time in left anterior oblique (LAO) position, and degrees of LAO angulation were independent predictors of PO head dose (p < .05).
the following diagrams explain it all: