Wiliam and John Hunter … Scottish brothers … born in 1718 and 1728; William was a dedicated educated person .. John never enjoyed books but was fund of natural observations … William established anatomy school .. John joined in … and under William’s guidance, john became a professional anatomist and teacher … John Hunter is well known for popliteal aneurysm repair. Potts noticed by that time that no matter how judiciously performed, proximal and distal ligation of aneurysm would not save the patient’s life. However, John realised that ligating very distally might be able to preserve the collaterals; hence his famous operation, published in London Medical Journal 1786. he decided to approach medially (not posteriorly). He did at St George’s Hospital. Hunter’s pupils were numerous, including Astley Cooper. However, his curiosity lead him to inoculate his own penis with a specimen taken from a patient suffering from urethritis. Years later, he developed syphilis and a syphilitic ascending aortic aneurysm. He then was informed about the appointment of a predecessor in St George’s hospital; he suffered a major angina which proved fatal. first vein graft – Alfred Exner from Austria (used canine external jugular vein) then Alexis Carrel from France (University of Lyon). They published their revolutionary idea of using vein as a bypass in 1906 (Surgery, Gyn, and Obst). Carrel designed the technique, that is still in use now: A rigid asepsis is absolutely essential for success. . . . The dissection of the vessel is not dangerous if the wall of the vessel is not crushed or roughly handled with metallic forceps of other hard instruments . . . it is necessary that these clamps [vascular] be smooth-jawed and not too strong in the spring . . . by using very sharp, rough needles, only extremely small wounds are made . . . great care is taken not to include fragments of the connective tissue layer in the line of suturing, and to obtain a smooth union and approximation of the endothelial coats. First clinical anastomosis, however, is sone/published by Jose Guyanese from Madrid. He used an adjacent popliteal vein piece to repair a popliteal aneurysm. to be continued …
The impact of intraoperative shunting on early neurologic outcomes after carotid endarterectomy
Kyla M. Bennett, MD, John E. Scarborough, MD, Mitchell W. Cox, MD, Cynthia K. Shortell, MD
Interesting to see the results:
There was no significant difference in the incidence of postoperative stroke/TIA between the two groups of this matched cohort (3.4% in the no-shunt group vs 3.7% in the shunt group; P = .64).
Analysis of a similarly well matched subgroup of patients with severe stenosis or occlusion of the contralateral carotid artery demonstrated a statistically nonsignificant increase in the incidence of postoperative stroke/TIA with the use of intraoperative shunting (4.9% in the no-shunt group vs 9.8% in the shunt group; P = .08).
My experience in no shunting has been good enough (no postoperative stroke so far)… however, the anaesthetist struggled [seriously] to control the BP where a contralateral stenosis existed .. making me ‘think’ that using a shunt makes life better for the anaesthetist (and patient) in the BP control, no more, no less …
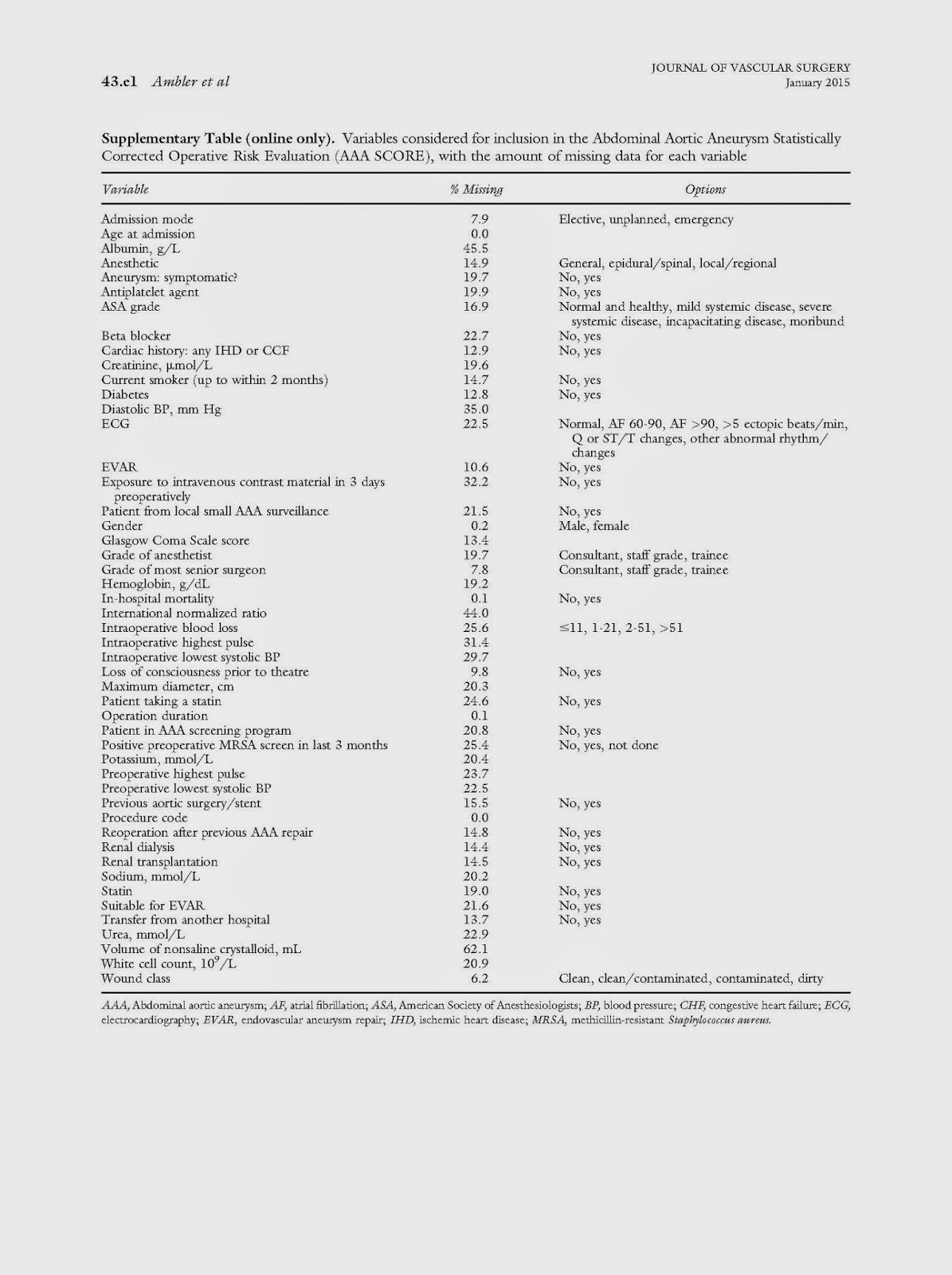
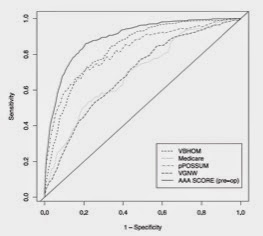
The Abdominal Aortic Aneurysm Statistically Corrected Operative Risk Evaluation (AAA SCORE) for predicting mortality after open and endovascular interventions
This is a good work aiming at predicting outcome following AAA surgery. The number of parameters used is large (49) but probably should anyway be available in any good quality vascular database.
The Score:
the calibration of this against other predictive models is shown in ROC curve:
This is quite good scoring system.. the main issue lies in the ability to apply it to practice; plus the cases were missing values exist … and of course how much this is going to add to the decision making …
It is also not unreasonable to say that the more factors you use, the better prediction you get … but practical life does not allow that … also, there are certain factors (duration of operation, wound class, etc.) that cn only obtained AFTER operating, not before … all make a scoring system like this not usable in decision making, but rather in (maybe) validating the performance of a unit/surgeon against others, after adjusting to risk (using the score). This is an important part of any quality assurance program in fact, and have certainly a role in current AAA practice.
Re: ‘“Spontaneous Delayed Sealing in Selected Patients With a Primary Type Ia Endoleak After Endovascular Aneurysm Repair.” Does Correcting the Picture Save the Life?’
In the original paper (1), All but one of the 15 primary type Ia endoleaks sealed spontaneously within 5 months. The disappearance of type Ia endoleaks resulted from improved graft wall apposition due to neck remodelling or thrombosis of the non-apposed neck segment.
However, although ruptures were not detected in the 14 patients, sac growth occurred in four (28.5%).1 In these patients known causes of sac growth were not detected by CT.
Biomechanical explanation (which does make sense indeed) is that If the barrier between the aneurysm sac and the systemic arterial circulation consists of thrombus only, systemic pressure can be transmitted through a clot, and it is known that mural thrombus on the surface of the aneurysm sac does not prevent rupture.(2) For this reason, a thrombotic barrier on the neck segment may eliminate type Ia endoleak but may not prevent rupture.
Solution– Maybe by introducing a stiff barrier that prevent from transferring the pressure down into the sac. Feng et al.3 documented results of patients treated by fibrin glue injection: one aneurysm related death and four aneurysm sac growths were detected in 48 cases during 45 months follow up.
_________________________________________
1) F.B. Gonçalvez, H.J.M. Verhagen, K. Vasanthananthan, H.J.A. Zandvoort, F.L. Moll, J.A. van Herwaarden
Spontaneous delayed sealing in selected patients with a primary type Ia endoleak after endovascular aneurysm repair
Eur J Vasc Endovasc Surg, 48 (2014), pp. 53–59
2) F.J. Veith, R.A. Baum, T. Ohki, M. Amor, M. Adiseshiah, J.D. Blankensteijn, et al.
Nature and significance of endoleaks and endotension: summary of opinions expressed at an international conference
J Vasc Surg, 35 (2002), pp. 1029–1035
3) J.X. Feng, Q.S. Lu, Z.P. Jing, Y. Yang, B. Nie, J.M. Bao, et al.
Fibrin glue embolization treating intra-operative type I endoleak of endovascular repair of abdominal aortic aneurysm: long-term result
Zhonghua Wai Ke Za Zhi, 49 (10) (2011), pp. 883–887
External Validation of Models Predicting Survival After Ruptured Abdominal Aortic Aneurysm Repair
EJVES Jan2015
What models are available nowadays, and how accurate they are?
Three models are been tested: updated Glasgow Aneurysm Score (GAS), the Vancouver scoring system, the Edinburgh Ruptured Aneurysm Score (ERAS), and the Hardman index
449 patients in ten hospitals with a RAAA (intervention between 2004 and 2011)
The updated GAS score – calculated with the formula: age (years) + 7 for cardiac comorbidity (defined as previous history of myocardial infarction, cardiac surgery, angina pectoris or arrhythmia) + 10 for cerebrovascular comorbidity (defined as previous history of stroke or transient ischemic attack) + 17 for shock (defined as an in hospital systolic blood pressure <80 mmHg) + 14 for renal insufficiency (defined as a pre-operative serum creatinine >160 μmol/L) + 7 for OR
predicted mortality rate (%) =
and the performance of GAS is as follows:
The Vancouver score – calculated with the formula: age (years)*0.062 + loss of consciousness (yes = 1/no = −1)*1.14 + cardiac arrest (yes = 1/no = −1)*0.6
predicted mortality rate (%) =
and the performance of Vancouver is as follows:
The ERAS score – calculated with the formula: +1 for best recorded in hospital Glasgow coma scale (GCS) <15, +1 for in hospital systolic blood pressure <90 mmHg, +1 for pre-operative hemoglobin level <5.6 mmol/L. A score of 0 or 1 corresponded with a predicted death rate of 30%, a score of 2 with a predicted death rate of 50%, and a score of 3 with a predicted death rate of 80%.
The Hardman index – calculated with the formula: +1 for age >76 years, +1 for in hospital loss of consciousness, +1 for a pre-operative serum creatinine >190 μmol/L, +1 for pre-operative serum hemoglobin level <5.6 mmol/L, +1 for electrocardiographic (ECG) ischemia (defined as ST segment depression greater than 1 millimeter or an associated T wave change determined by a senior cardiologist [RJGP]). A score of 3 or more corresponded with a predicted death rate of 100%.
OVERALL RESULTS:
The AUC of the updated GAS was 0.71 (95% confidence interval [CI] 0.66–0.76), of the Vancouver score was 0.72 (95% CI 0.67–0.77), and of the ERAS was 0.58 (95% CI 0.52–0.65).
After recalibration, predictions by the updated GAS slightly overestimated the death rate, with a predicted death rate 60% versus observed death rate 54% (95% CI 44–64%).
After recalibration, predictions by the Vancouver score considerably overestimated the death rate, with a predicted death rate 82% versus observed death rate 62% (95% CI 52–71%).
Performance of the Hardman index could not be assessed on discrimination and calibration, because in 57% of patients electrocardiograms were missing.
Decision making
The decision to withhold intervention in patients with a RAAA can be very difficult. Only extremely reliable models can be useful in clinical decision making and in identifying patients in whom withholding intervention might be considered.
For this purpose, a cut-off value for the predicted death rate was set at ≥95%. If the death rate was to be predicted accurately at 95%, the number needed to treat (NNT) would be 20. This cut-off value is arbitrary and could also have been 90% (NNT of 10) or 99% (NNT of 100). Different cut-off values can be used depending on the clinical situation.
None of the prediction models met the criterion of identifying patients in whom to withhold intervention. This disappointing conclusion is in agreement with previous validation studies.21, 22 and 23
Currently, the prediction models have insufficient accuracy to evaluate the chances of successful intervention and future studies should focus on improvement towards this aim. The usefulness of current prediction models lies in case mix comparisons between hospitals, and in a tailored prognosis for patients and relatives.
Randomized clinical trial to evaluate mental practice in enhancing advanced laparoscopic surgical performance Mental practice, the cognitive rehearsal of a task without physical movement, is known to enhance performance in sports and music. This is now tested (in a randomised trial setting) on performing laparoscopic surgery in bariatric. and .. there is a difference between the operator’s performance; which is significant enough (p=0.011).
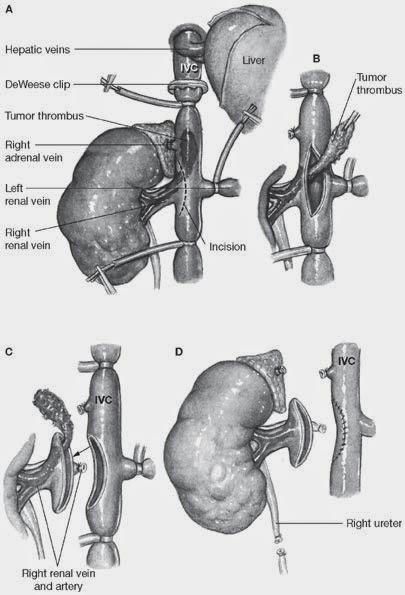
Combined vascular resection and reconstruction during hepatobiliary and pancreatic cancer surgery. In old days, once a cancer has invaded the IVC/portal vein, it is palliative treatment only -mortality rate of resection was 6% and 5yr survival was 27% (1999). However, recent reports from major vascular centres (Leads, Paris) has shown much better outcome, with mortality rate of 11-14% and survival rate of 40% in 5yrs following IVC resection. Technical point: IVC can be ligated unless there is not enough collateral developed in before, or there is haemodynamic instability. Portal vein resection as part of pancreatectomy is now widely regarded as a safe and feasible procedure with acceptable morbidity and mortality rates. Combined portal vein resection with pancreatectomy should be considered where there is a suspicion of invasion of the portal vein to achieve clear resection margins on the basis of preoperative imaging rather than making the decision purely on operative findings. Unlike the situation with hepatic resections, combined arterial resections involving the coeliac axis, at least in the context of distal pancreatectomy, have been reported without a marked increase in surgical mortality.A variety of substitutes for venous reconstruction have been reported. Jugular, external iliac vein, great saphenous vein, left renal and umbilical veins, as well as synthetic grafts have all been used for portal vein reconstruction.here are few diagrams of the technique: